
… ..
..
 …
…

… ..
..

..
…
…
…
…
…
…
…
…
..
…
…
…
..
.. …
…

…
…
…
…
…
… ..
..

…..
…
…..
..
…
…
…
…
…
…
…
…
..
…
…
…
..
..…
…
…
…
…
…
…..

Visions from life on foot in a city that never sleeps.

…

…
…

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…



…

…

…

…

…
…

…

…

…

…

…

…

…

…

…


…

…

…

…

…

…

…

…

…

…

…

…

…


…

…

…

…


…



Photo: UNICEF Cambodia, Antione Raab
Chronic diseases have risen to the top as the leading causes of death and disability worldwide. Once considered a problem for the elderly in developed nations has now become a global pandemic. In 2012, over 50% of adults in the U.S. had one or more chronic disease. By 2020, chronic diseases will account for 73% of all deaths across the globe. However, nearly 80% of these deaths will occur in developing countries. The inequitable distribution of resources and access to healthcare will ultimately result in the greatest harm to the most vulnerable populations.
Cambodia, like many other developing nations, is experiencing a rise in noncommunicable diseases (NCDs), pervasive and long-term ailments that include cancer, chronic respiratory disease, diabetes mellitus, and cardiovascular disease. There are various determinants that can contribute to the rising prevalence of NCDs, including genetics, lifestyle choices, and the environment. While negative behaviors can often be changed through targeted public health interventions, ultimately, the social and physical environments must also change in order to support individuals in making healthier choices.
From a macro perspective, the current health status of Cambodia’s population is greatly influenced by its economic state of development and health care infrastructure. Ranked as a low-income country by the World Bank, Cambodia has a Gini coefficient of 31.8 and a Gross National Income (GNI) of $2,890 per capita. 15 For the population of 14,865,000, inequity is high across socio-economic groups and noticeably different between rural and urban areas. This unequal distribution of wealth and resources inevitably impacts access to care. For instance, greater health care barriers are faced by 80% of the population, who populate rural and remote areas with minimal access to medical treatment facilities. Additionally, poverty is another barrier to care, as 45.9% of the population lives on less than $1.25 per day. 12 As a result, nearly half of Cambodia’s population struggles to obtain daily necessities and is unable to afford the high cost of medical care, which accounts for over 60% of total health expenditures. 12

Photo: Global Witness, Chean Chenda

Photo: Daily Mail.uk
It has also been speculated that the lack of access to health care has contributed to the country’s lower life expectancy at birth, which according to the World Health Organization (WHO) is 75 years for females and 70 years for males. 12 Furthermore, the crude birth rate is 25 live births per 1000 people, while the crude death rate is 6.70 deaths per 1000 people. 17 Additionally, the fertility rate is 2.9 births on average per woman over a lifetime. 11 All of these factors are contributing to the rising demand for health care to both meet the needs of the growing population and minimize preventable deaths. 11
The greatest suffering is experienced in rural communities, which lack access to available health care providers to adequately meet their needs. In 2008, there were only two physicians and eight nurses/midwives available for every 10,000 people living in rural areas. 17 Additionally, by 2011 there were only eight health facilities and 72 hospital beds available for every 100,000 people. 17 However, during the same year, there were 710 new nursing graduates and 134 new medical school graduates. 13 This illustrates that while the number of nurses entering the health care workforce was and is promising, the shortage of physicians and lack of available health care facilities still remains problematic.
In addition to a lack of medically trained providers, rural communities face numerous obstacles in accessing care. For one, quality is a major concern. A substantial part of the population, approximately 21%, receives care from the private non-medical sector, which is comprised mostly of traditional and religious healers. 13 This is concerning since most of these private facilities are not actively regulated, thus, making the quality of assurance questionable. Similarly, 49% of medical treatments occur through private facilities where quality assurance and regulation is minimal. 17 As a result, this negatively impacts the ability to prevent (via screening), treat, and manage NCDs for the most affected groups (e.g. low socio-economic status). This environmental barrier must change in order to provide greater access to health care nationwide.
While Cambodia has many environmental obstacles, there are also several opportunities that can be utilized to improve public health. For instance, the increasing rates of education can be a means to share knowledge and facilitate change. Currently, the primary school enrollment rate is at 98% and the total adult literacy rate is at 77.6%. 12 Education may serve as an outlet to inform the public on the negative consequences of poor behaviors (e.g. smoking) and how to alternatively make healthier choices.

Photo: UNDP
Another opportunity is to utilize the international aid coming into Cambodia. In 2010, contributions targeting health care reached $199 million.12 However, more than half of this aid went towards treating communicable diseases, such as HIV, TB and Malaria. A focus on infectious diseases has swept across the international community, non-governmental organizations (NGOs) and the Cambodian government. Multi-sectoral collaboration (including many of the 30 aid partners), has given rise to new policies, which focus monetary funds primarily on lowering infectious disease rates. The implications of such an agenda is that the prevention and treatment of many noncommunicable diseases may be overlooked.
In order to develop a broad and accessible healthcare system that benefits all people, a stronger emphasis needs to be placed on the prevention and treatment of NCDs. Based on current rates, chronic diseases will have the greatest impact on population health overtime. The result of this focus will inevitably be perceived in the near and far future. Ultimately, a greater percentage of the population will benefit from access to healthcare and an improved standard of living overall.

Photo: Buffalotours
Studies show that chronic diseases are increasing in prevalence, while communicable, maternal, neonatal, and nutritional causes of disability-adjusted life years (DALYs) are declining. 18 DALYs represent the number of healthy years lost to due disability or premature death. According to the World Health Organization’s 2014 Noncommunicable Diseases Country Profile on Cambodia, NCDs caused 44,200 deaths accounting for 52% of all total deaths. 15 By comparison, communicable, maternal, perinatal and nutritional conditions only accounted for 31,450 deaths or 37% of total deaths. 15 This trend has been quantified by various studies, which provide evidentiary support for why more agency should be placed towards the prevention, treatment and management of NCDs.
The Global Burden of Diseases, Injuries, and Risk Factors Study compared changes in disease rates in Cambodia from 1990 to 2010. 18 This study determined the greatest burden by the absolute number of DALYs lost and then ranked each disease from 1 (best) to 15 (worst) according to the age standardized DALY rates. In 1990, the leading causes of DALYs lost were due to lower respiratory infections (rank: 8), followed by diarrheal diseases (rank: 3), and then malaria (rank: 8). In 2010, the leading cause of DALYs lost still remained to be lower respiratory infections but with a lower ranking of 4. However, the disease with the second greatest burden was now ischemic heart disease (rank: 13), followed by stroke (rank: 12). Overall, from 1990-2010 lower respiratory infections declined by 50% while ischemic heart disease increased by 75% and stroke increased by 55%. 18 Additionally, diarrheal disease, which was once the leading cause of burden, showed the greatest decrease in DALYs by 50%. 18 Similarly, other communicable diseases have had great reductions in DALYs, such as malaria (40%), meningitis (25%), and tuberculosis (10%). 18 In contrast, from 1990-2010, many NCDs have increased in disease burden, such as diabetes (110%), Cirrhosis (85%), COPD (25%), and other cardio and circulatory diseases (20%). 18 This shows that infectious diseases are declining while NCDs are rising in prevalence and severity.

Photo: Paula Bronstein, Getty Images
Since 2010, the prevalence of NCDs has continued to rise. In 2014, 7,400 people suffered from a stroke, while diabetes prevalence rose to 229,000. 14 The annual environmental burden for cardiovascular disease was calculated at 4 DALYs per 1000 capita. 14 In addition, cancer now affects 6,842 males and 8,374 females in Cambodia. 21 The most common cancers in males include liver (1,444 cases), lung (796 cases), and colorectal cancer (445 cases). 21 By comparison, the most common female cancers are of the cervix uteri (1,512 cases), breast (1,255 cases), and liver (820 cases). 21 According to the WHO, the annual burden of lung cancer is 0.3 DALYs per 1000 capita, while for all other cancers is 2.0 DALYs per 1000 capita. 14 Overall, the burden of cancer is high, which means that there is a large number of preventable deaths that are associated with unhealthy environments.
NCDs cause tremendous suffering, especially for individuals who go untreated. This is compounded with the fact that a majority of NCD deaths occur in individuals under 60 years old, with males accounting for 56.2% and females accounting for 34.8%. 20 This is highly problematic since most NCD deaths impact the working population, which reduces the labor force in Cambodia. The economic impact is high, as the productivity losses associated with absences, accidents and disability were found to be 400% greater than the cost of treatment.26 Ultimately, the economy would benefit from increased population treatment for NCDs. However, when families have to contend with the early death and/or disabilities of a household financial provider, the families are pushed into poverty due to the high cost of chronic treatment. Therefore, it is clear that more cost effective prevention and treatment options are needed.

Photo: MSAVLC

Photo: ICRC
There are various underlying socio-economic, cultural, political, and environmental determinants of NCDs. For instance, globalization and urbanization have contributed to more sedentary lifestyles and the wide distribution of highly processed foods. Low-income households are large consumers of these high calorie, low nutrient items, due to their extensive availability and low costs. Similarly, current government policies in Cambodia make cigarettes affordable and widely available. For instance, at current rates, a pack of Marlboro cigarettes costs only $1.15, which is surprisingly less than the cost of a liter of Milk selling at $1.99. 25 The outcome is a physical environment that supports unhealthy behaviors, thus, enabling individuals to engage in common risk factors that are responsible for many chronic diseases.
This is evident in the high rates of modifiable risk factors such as unhealthy diets, physical inactivity, and tobacco use, as well as intermediate risk factors such as high blood pressure and obesity in the population. Currently, the prevalence of daily tobacco smoking among Cambodians is at 30%. 12 Also, 12.1% of the population is overweight, 11.2% are physically inactive, 2.1% are obese, and 27.6% have high blood pressure. 20 Furthermore, alcohol consumption is high at 5.5 liters per capita. 15 As such, it is no surprise that the leading risk factors that accounted for the greatest burden of disease in 2010 were dietary risks, household air pollution from solid fuels, and tobacco smoking, amongst others. 18
Of the total risk factors, dietary risks accounted for 9%, household air pollution accounted for 8.5% and smoking accounted for 7%. 18 These risk factors lead to cardiovascular and circulatory diseases, diabetes, cancer, diarrhea, lower respiratory infections, chronic respiratory diseases, and many other NCDs. Public health efforts should focus on educating and empowering the population on methods to minimize the risk of developing these high burdening diseases. For instance, behavior modification could target the four main modifiable risk factors, which include tobacco smoking, alcohol consumption, dietary risks, and physical inactivity. Engaging in these behaviors can drastically impact health. For example, smokers are 20 times more likely to develop lung cancer than those who have never smoked. 26 Similarly, inactivity and obesity resulting from poor diet increases the risk of death by at least 50%. 26 Thus, focusing policy and public health interventions on lowering these risks would dramatically aid in reducing NCDs.

Photo: Phnom Penh Post
In order to promote population health and well-being, education efforts should focus on the most wide spread and damaging habits. Scientific evidence has shown this to be smoking, alcohol consumption, physical inactivity, and unhealthy diets. 18 One method to change these behaviors is through policy change. For instance, public health interventions can be implemented in primary schools, which have high attendance rates and therefore, serve as prime locations to educate children on nutrition early on. Also, government subsidies for fruits and vegetables may help alleviate the financial barrier for those unable to afford fresh produce. Additionally, the Cambodian government could legislate to follow global agreements by supporting the commitments under the Framework Convention on Tobacco Control (FCTC). Furthermore, public smoking bans in certain areas (e.g. schools) and tighter advertising regulations may also help reduce current smoking rates. Overall, education should approach the four main risk factors with an aim to change social norms, all the while implementing policies that promote a healthier physical environment.

Photo: Khmer Times

Photo: Financial Times
A greater medical workforce is needed to keep up with population growth and the expanded coverage of care. One method to increase healthcare professionals, such as physicians and nurses, is by providing financial incentives (e.g. loan forgiveness) for students to pursue healthcare in Cambodia. However, before newly trained professionals enter the field, there needs to be a national standard for quality of care that is implemented and assured. In order to do so, the health workforce strategy must be revised, and training (both pre-service and in-service) must be strengthened. 12 Also, capacity building and knowledge sharing is needed in order to effectively spread information on standard treatment protocols and quality accreditation. This must occur across various health care groups, including the private sector and universities.
One reason NCDs are negatively impacting Cambodia’s population is due to the lack of access to affordable quality care for screening, treatment, and disease management. However, the government has been making changes towards improving access. The Cambodian Government recently implemented the second Health Strategic Plan 2008-2015 (HSP2). Focus has now moved towards implementing the National Strategic Development Plan (NSDP) 2014-2018, which aims to improve population health and access to resources in a sustainable fashion. 12 One positive outcome is the expansion of Health Equity Funds (HEFs), which now cover 80% of the poorest people in the country and helps reduce the financial obstacles to receiving care. However, 20% of the poorest population still lacks access and the financial resources to obtaining quality healthcare. Therefore, this underserved population should be targeted through outreach services and facility based coverage. Strengthening and coordinating the resources of NGOs to assist in supporting the WHO’s Cooperative Strategic Agenda (2008-2015) may help achieve full coverage. 12 This would also support the development of a national social health protection policy and financing mechanisms that target the poor.
In addition, low-cost medications should be provided to high-risk patients (e.g. hypertensive) or those requiring long-term treatment due to chronic disease (e.g. cancer). With advancing technologies, cost effective strategies for NCD prevention and treatment are becoming more common. Optimism is high, as new strategies are estimated to prevent 80% of diabetes and global heart disease in the future. 26 For instance, high blood pressure can be effectively managed with medication at a low cost of only a few cents per day. 26
Furthermore, with expanded coverage, screenings for disease must also increase. This is vital, since many NCDs are not curable, and most have a slow onset and long duration. Thus, early detection combined with treatment and management will provide the greatest benefit for patients. This has occurred in many high-income countries which have had increased rates of survival due to cancer treatments combined with early detection and screening. 26 For instance, the 50-year relative survival rate for all cancers diagnosed in the US from 1975-1977 was 49% compared to 68% from 2004-2010, reflecting advances in treatment and early diagnosis. 24
Overall, a serious problem faces Cambodia. On the one hand, policy makers must consider how to manage the growing element of NCDs and how to reduce the negative physical, financial, and national burden that they have on the population. On the other hand, decision makers must utilize the countries current resources of international aid and upcoming policy reform in order to emphasize education and implement broad-based healthcare availability. Ultimately, in order to reduce the impact of NCDs in the future and improve the health of Cambodia’s population, policy efforts should focus on expanding healthcare coverage, reducing treatment costs, and both increasing and improving screening, treatment, and disease management.

Photo: UNICEF Cambodia
REFERENCES
APPENDICES
| Indicator | Data | Latest year | Source |
| Total population | 15,205,539
14,865,000 |
2013
2014 |
11 15 |
| Crude death rate (per 1000) | 6.70 | 2004 | 17 |
| Crude birth rate (per 1000) | 25 | 2004 | 17 |
| Life expectancy at birth (yrs) |
72 (Both Sexes) 75 (Female) 70 (Male) |
2012 | 12 |
| Total fertility rate | 2.9 per woman | 2013 | 11 |
| Total adult literacy (%) | 77.6% | 2008 | 12 |
| School Enrollment rate | 98% net, primary | 2012 | 3 |
| Ranked low, middle or high income? | Low-income | 2012 | 3 |
| GNI per capita ($) | $2,890 | 2013 | 13 |
| Gini coefficient | 31.8 | 2011 | 3 |
| Population living below $1.25/day (%) | 45.9% | 2010 | 12 |
|
Major imports |
Refined Petroleum (10%) Light Rubberized Knitted Fabric (10%) Other Synthetic Fabrics (3.6%) Raw Sugar (2.1%) Gold (2%) |
2014 | 3 |
|
Major exports |
Postage Stamps (14%) Knit Sweaters (12%) Knit Women’s Suits (7.7%) Non-Knit Women’s Suits (5.5%) Non-Knit Men’s Suits (5.3%) |
2014 | 3 |
| % deaths due to infectious disease | 20.16% | 2011 | 8 |
| % deaths due to NCDs | 52% | 2014 | 15 |
| Top 3 diseases (in terms of deaths): 1. Ischemic heart disease (10.1%), 2. TB (9.6%), 3. Stroke (8.7%) | 8.5
8.2 7.4 (Thousands) |
2012 | 11 |
| Top 3 diseases (in terms of DALYs lost): 1. Lower respiratory infections, 2. Ischemic heart disease, 3. Stroke |
6,600 (Age standardized DALYs 1-15: 4) 8,500 (Age standardized DALYs 1-15: 13) 7,400 (Age standardized DALYs 1-15: 12) |
2012, Age stand. DALYs: 2010 |
18 11 |
| DALYs lost (%) | N/A | ||
|
Top 3 causes of DALYs lost: 1. Maternal, neonatal, nutritional, 2. Other NCDs (non-malignant neoplasms; endocrine, blood and immune disorders; sense organ, digestive, genitourinary and skin diseases; oral conditions; and congenital anomalies), 3. Cardiovascular diseases and diabetes Risk Factors accounting for most disease burden: 1. Dietary Risks, 2. Household Air Pollution, 3. Smoking |
~ 820,000
~ 610,000 ~ 600,000 9% DALYs 8.5% DALYs 7% DALYs |
2012
2010 |
11, 18 |
| Indicator | Data | Latest year | Source |
| Environmental Health | |||
| Environmental Burden of Disease (%) | Deaths: 25% of total burden | 2004 | 14 |
| Top 3 greatest contributors to environmental burden of disease (DALYs): 1. Diarrhea, 2. Respiratory Infections, 3. Unintentional injuries (other than road traffic) |
27 18 5.9 (DALYS/1000 capita) per year |
2004 | 14 |
| Deaths due to Indoor Air Exposure (Deaths/year) | 6,600 deaths/year | 2004 | 14 |
| Deaths due to Outdoor Air Exposure (Deaths/year) | 300 deaths/year | 2004 | 14 |
| Global Climate Change Threat | N/A | ||
| Water and Sanitation | |||
| Water Situation (scarcity) | 33% people lack access to safe water | 2008 | 27 |
| Population using improved water and sanitation (%) |
Sanitation: 22% (Rural) 76% (Urban) Overall: 67% Water: 61% (Rural) 90% (Urban) |
2011 | 12 |
| Burden of Disease from Diarrheal Disease | 27 DALYs/1000 capita (per year) 10,000 children die/year |
2004 2014 |
14 27 |
| Indicator | Data | Latest year | Source |
| Maternal health | |||
| Antenatal coverage, at least once (%) | 89% | 2010 | 1 |
| Antenatal coverage, at least four times (%) | 59% | 2010 | 1 |
| Skilled attendant at birth (%) | 71% | 2010 | 12 |
| Contraceptive prevalence (%) | 51% | 2007 | 11 |
| Maternal mortality ratio | 250/100,000 live births
170/100,000 live births |
2010
2013 |
12 |
| Child health | |||
| Annual number of under-five deaths | 40/1000 (38/1000 live births ) * 388,880 births = 14,777.44 deaths |
2012 2013 |
12 11 |
| Infant mortality rate | 45/1000 live births | 2010 | 17 |
| Child mortality rate | Prob. of dying before age 15: M: 20%, F: 16% | 2012 | 11 |
| Neonatal mortality as proportion of all under-five mortality | (18/1000 live births) * (38/1000 live births) = 0.47368 deaths (6,999.77 deaths/year)
18/1000 live births |
2012
2013 |
12 |
| Nutrition | |||
| Percent of babies born with low birth weight | 8.2% | 2012/13 | 17 |
| Children exclusively breastfed < 6 months (%) | 73.5% | 2012/13 | 17 |
| Children still breastfeeding 20-23 months (%) | 3.51% | 2010 | 1 |
| Children moderately or severely underweight (%) | < 5 yrs old: 28% | 2012/13 | 17 |
| Children moderately or severely wasted (%) | 11% | 2010 | 1 |
| Children moderately or severely stunted (%) | 39.5% (under 5 years old: 40%) |
2012/ 2013 2014 |
17 12 |
| Vitamin A supplementation full coverage (%) | 71% | 2010 | 1 |
| Households consuming iodized salt (%) | 84% | 2010 | 1 |
| Children 1-year-old receiving measles immunization (%) | 90% | 2007 | 11 |
| Indicator | Data | Latest year | Source |
| Major Diseases | |||
| Total # of NCD deaths | 44,200 | 2014 | 15 |
| % of NCD deaths to people under 60 yrs. | Males: 56.2% Females: 34.8% | 2008 | 20 |
| Stroke | 7,400 Age Standardized Death rate: 101.49/100,000 ppl |
2014 2011 |
15 |
| COPD | 1.1 DALYs/1000 capita per year | 2004 | 14 |
| Diabetes prevalence | 229,000 | 2014 | 22 |
| Cancer Deaths & Cases |
Deaths: 13% = 11,050 Cases: M: 6842 F: 8374 |
2014 2012 |
15
21 |
| Top 3 cancers (males) 1.Liver, 2. Lung, 3. Colorectal |
1444 cases 796 cases 445 cases |
2012 | 21 |
| Top 3 cancers (females) 1. Cervix, 2. Breast,3. Liver |
1512 cases 1255 cases 820 cases |
2012 | 21 |
| Risk Factors | |||
| Current Daily Tobacco Smoking prevalence (%) overall, males, females |
30% 42% 3% |
2014
2011 |
12
15 |
|
Physical inactivity overall, males, females |
11.20% 11.40% 11.10% |
2008 | 17 |
| Alcohol consumption per capita | 5.5 liters | 2010 | 15 |
| Overweight (%) overall, males, females |
12.1% 10.8% 13.2% |
2008 | 20 |
|
Obesity (%) overall, males, females |
2.1% 1.5% 2.7% |
2008 | 20 |

A city of jagged hills sprayed with colors of pastel from the eclectic mix of Victorian and modern architecture. An evolving cultural scene, from the height of the hippie movement and 90’s grunge to the technological revolution of today.

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…

…
 …
…

…

…
…

…

…

…

…

…

…

…


A concrete union of tribal villages in the modern hub of capitalism.
…

…

…

…

..

…

…

…

…

…
…

…

…

…

…

…

…

…

…

…

…

…

…

..
..




…
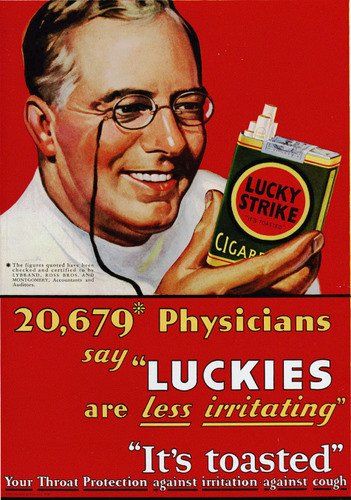
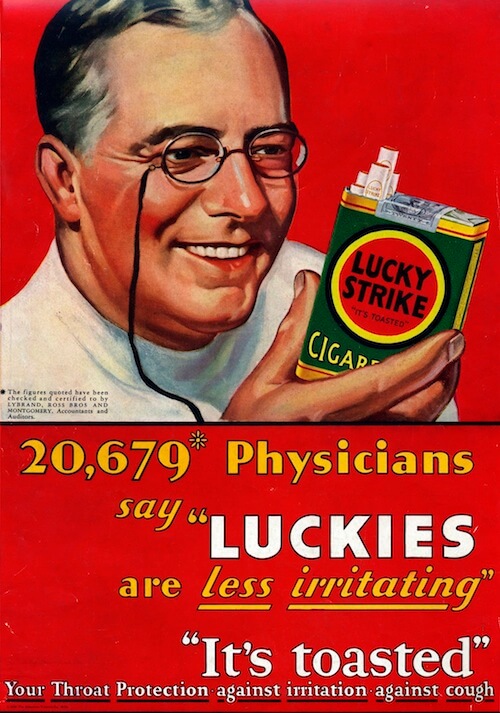
“Tobacco is the only legal drug that kills many of its users when used exactly as intended by manufacturers” (15).
According to the World Health Organization (WHO), tobacco use is responsible for six million deaths each year (15). This includes an estimated 600,000 people who die from second-hand smoke. Health outcomes include death and/or disability from chronic diseases, such as cancer, stroke and chronic respiratory diseases. Additionally, smoking increases the risk of death from infectious diseases.
Overwhelming evidence suggests that tobacco marketing greatly influences tobacco use and initiation (3-5). As such, bans on tobacco marketing can greatly reduce individual tobacco use.
Tobacco use in many high income countries is decreasing rapidly. This is due to government marketing bans and increased public education about the harms of smoking. In contrast, the prevalence of smoking is increasing in many middle- and low-income countries. According to the WHO global report on trends in tobacco smoking 2000-2025, males are more likely to smoke than females, and the prevalence is rising most dramatically in the African Region and the Eastern Mediterranean Region (13).
Photo by: Merinews

Photo by: World Not Tobacco Day Africa
Table 1. Age-standardized prevalence of current tobacco smoking among persons aged 15 years and older (14,16).
| Country | CURRENT TOBACCO SMOKING (%) | |||||
| Year 2000 | Year 2015 | |||||
| Men | Women | Both sexes | Men | Women | Both sexes | |
| High-income | ||||||
| Canada | 29.3 | 27.5 | 27.5 | 17.7 | 12.2 | 14.3 |
| Sweden | 32.8 | 32.9 | 32.9 | 20.4 | 20.8 | 20.6 |
| Upper-middle-income | ||||||
| China | 56.2 | 3.3 | 30.4 | 47.6 | 1.8 | 26.3 |
| Lower-middle-income | ||||||
| India | 33.8 | 5.7 | 20.2 | 20.4 | 1.9 | 11.0 |
| Pakistan | 35.2 | 7.5 | 21.8 | 41.9 | 3 | 22.9 |
| Low-income | ||||||
| Zimbabwe | 29.8 | 2.7 | 16.1 | 31.2 | 2.1 | 16.65 |
Tobacco marketing is 81 times greater in Pakistan, India and Zimbabwe than in the United Arab Emirates, Canada and Sweden (7).
In 2003, member states of the World Health Assembly adopted the Framework Convention on Tobacco Control (FCTC) (6). This agreement provided 180 nations with evidenced-based steps to minimize tobacco sales and ban tobacco marketing. This legally binding treaty even provided agricultural alternatives to those growing tobacco, so as to minimize the economic hardships faced by local producers. Nearly 13 years later, what is the present state of tobacco marketing trends?
A recent study led by the World Health Organization examined the global tobacco marketing environment by comparing 462 communities located in 16 low-, middle- and high-income countries (1). Researchers found that exposure to tobacco marketing is 81 times greater in Pakistan, India and Zimbabwe than in the United Arab Emirates, Canada and Sweden (7). Additionally, the tobacco industry is targeting poor urban youth in developing countries (10-12). This is due to cheaper marketing costs and the greater potential to reach more people in densely populated regions. Furthermore, according to the WHO study (1), high levels of tobacco marketing (e.g. posters, print media and cinema) was even found in 14 middle- and low-income countries that had ratified the FCTC. Countries that ratified this agreement were required to implement a comprehensive ban on tobacco advertising, promotion and sponsorship. However, many developing countries are lacking in agency and governmental capacity to fully implement the recommendations of FCTC (2). This is worsened by the alarming influence of the tobacco industry in lobbying their interests (8,9).
Governments, NGOs, and other key stakeholders need to take a stand against the tobacco companies. Media and advocacy work must continue to focus on the populations currently being abused by corporate greed. Urban youth in developing countries are the greatest target of the tobacco industry, and therefore, should become a major focus for public education initiatives about the harmful effects of tobacco use. Nations across the globe have already taken a positive step forward by agreeing to the Framework Convention on Tobacco Control. People must now take the next step by supporting fellow nations in implementing this agreement to ban tobacco marketing. Financial resources, capacity building and continued media attention are needed now more than ever. A healthier and more equitable world is possible in the future, but there is a long way to go.
…
…
…
REFERENCES
1) http://www.who.int/bulletin/volumes/93/12/15-155846.pdf
2) http://www.triplepundit.com/2015/12/developing-countries-targeted-tobacco-marketing/
3) The role of the media in promoting and reducing tobacco use. NCI Tobacco Control Monograph No.19. Bethesda: National Institutes of Health; 2008.
4) DiFranza JR, Wellman RJ, Sargent JD, Weitzman M, Hipple BJ, Winickoff JP; Tobacco Consortium, Center for Child Health Research of the American Academy of Pediatrics. Tobacco promotion and the initiation of tobacco use: assessing the evidence for causality. Pediatrics. 2006 June ;117(6):e1237–48. doi: http://dx.doi.org/10.1542/peds.2005-1817 PMID: 16740823
5). Pierce JP, Choi WS, Gilpin EA, Farkas AJ, Berry CC. Tobacco industry promotion of cigarettes and adolescent smoking. JAMA. 1998 Feb 18;279(7):511–5. doi: http://dx.doi.org/10.1001/jama.279.7.511 PMID: 9480360
6) World Health Organization. Parties to the WHO Framework Convention on Tobacco Control. Updated 26 July 2016. Retrieved from http://www.who.int/fctc/signatories_parties/en/
7) Gilmore, Anna. Big tobacco targets the young in poor countries – with deadly consequences. The Guardian. 1 December 2015. Retrieved from https://www.theguardian.com/global-development/2015/dec/01/big-tobacco-industry-targets-young-people-poor-countries-smoking
8) AMESCA regional plan 1999-2001. London: British American Tobacco: 1999. Available from: http://legacy.library.ucsf.edu/tid/kiz13a99/pdf [cited 2014 Jul 15].
9) Lee S, Ling PM, Glantz SA. The vector of the tobacco epidemic: tobacco industry practices in low and middle-income countries. Cancer Causes Control. 2012 Mar;23(1) Suppl 1:117–29. doi: http://dx.doi.org/10.1007/ s10552-012-9914-0 PMID: 22370696
10) Perlman F, Bobak M, Gilmore A, McKee M. Trends in the prevalence of smoking in Russia during the transition to a market economy. Tob Control. 2007 Oct;16(5):299–305. doi: http://dx.doi.org/10.1136/tc.2006.019455 PMID: 17897987
11) Gilmore AB, Radu-Loghin C, Zatushevski I, McKee M. Pushing up smoking incidence: plans for a privatised tobacco industry in Moldova. Lancet. 2005 Apr 9-15;365(9467):1354–9. doi: http://dx.doi.org/10.1016/S0140- 6736(05)61035-5 PMID: 15823388
12) Neuwirth B. Marketing channel strategies in rural emerging markets: unlocking business potential. [Internet]. Evanston: Kellogg School of Management; 2012. Available from: http://www.kellogg.northwestern. edu/~/media/files/research/crti/marketing%20channel%20strategy%20 in%20rural%20emerging%20markets%20ben%20neuwirth.ashx [cited 2013 Aug 15].
13) World Health Organization. Global Health Observatory (GHO) data: Prevalence of tobacco smoking. Accessed 1 December 2016. Retrieved from http://www.who.int/gho/tobacco/use/en/.
14) World Health Organization. Prevalence of tobacco smoking. Accessed 1 December 2016. Retrieved from http://gamapserver.who.int/gho/interactive_charts/tobacco/use/atlas.html
15) World Health Organization. WHO global report on trends in tobacco smoking 2000 – 2025. Updated 2016. Accessed 1 December 2016. Retrieved from http://www.who.int/tobacco/publications/surveillance/reportontrendstobaccosmoking/en
16) World Health Organization. WHO global reports on trends in prevalence of tobacco smoking 2015. (2015). Retrieved from http://apps.who.int/iris/bitstream/10665/156262/1/9789241564922_eng.pdf?ua=1

…
Over 1,000 women are brutally murdered in Pakistan each year.
October 6, 2016

Photo by: Borgen Magazine
Pakistan is a patriarchal society where women’s behaviors are traditionally limited by cultural restrictions in order to preserve their chastity. Any deviant behavior is therefore deemed immoral and brings dishonor upon the family. Consequently, women labeled as deviant are often murdered by male relatives or neighbors in order to restore familial honor and reputation within the community (1). These brutal acts of murder are known as honor killings. Each year, over 1,000 women in Pakistan are murdered in the name of honor.
While “immoral behavior” includes infidelity, it also encompasses a range of unexpected behaviors. For instance, women are often murdered for being raped, refusing an arranged marriage, dressing “inappropriately” or acting flirtatious. It can also be warranted by familial quarrels over property ownership, inheritance issues, or a woman’s desire to marry for love. Many times women are even murdered on the basis of suspicion alone (2).
…

Photo by: Gospel Herald
Human rights groups have been pressuring the Pakistani government to put an end to honor killings. However, authorities have been unsuccessful and have often even turned a blind eye. In many cases, murders are not even investigated, leaving perpetrators free from prosecution (3).
…

Photo by: BBC
This issue has gained international attention, especially with the rising number of high-profile honor killings this year. One such case was Qandeel Baloch, a Pakistani social media star, who was strangled to death by her brother in July. Pakistani filmmaker and activist, Sharmeen Obaid, also heightened international attention towards this issue in her Academy Award winning documentary, A Girl in the River: The Price of Forgiveness.
In response to the rising campaigns for women’s rights, the Pakistani government passed a bill ensuring that killers receive a mandatory life sentence (4). Previously, a killer could be pardoned for murder if he gained forgiveness from the victim’s family. This new legislation no longer allows freedom from impunity. Even still, it remains uncertain whether this law is enough to deter honor killings. However, activists everywhere are celebrating this new step in the right direction towards ending violence against women.
…

Honor killing suspects are blind folded before their court hearing. (Photo by: CNN)
…
REFERENCES

Life is made of stories.
Violence, corruption, abuse.
Somewhere between past & present lies truth.
Discover truth and you will find power,
The power to change the world.
The power to fight for freedom, justice & hope.
By exposing the dark side of the human condition,
There may be light.
As truth is enlightenment.
And people have the power,
The power to change the world.

{kind=link}
{kind=link}
{kind=link}